Normal - Abnormal Breathing Pattern - ppt download
5 (460) · $ 11.99 · In stock
Introduction Lungs major function Provide continuous gas exchange between inspired air and blood in the pulmonary circulation
Pulmonary Medicine Department. Ain Shams University.
Provide continuous gas exchange between inspired air and blood in the pulmonary circulation.
Nasopharynx. Larynx. Trachea. Bronchi. Bronchioles. Alveoli.
Upper airway filters airborne particles, humidifies and warms inspired gases. Lower airway serves for gas exchange.
Pulmonary circulation for gas exchange with the alveoli (pulmonary artery with subdivisions) Bronchial arteries arising from descending aorta supplies lung parenchyma.
Controlled in the brain stem. Mediated by muscles of respiration. Diaphragm primary muscle of inspiration. Accessory muscles of inspiration. SCM. Scalenes. Intercostals. Expiration is a passive process from elastic recoil of lung and chest wall, with passive diaphragm relaxation.
Pressure gradient required to generate air flow. Diaphragm contracts, descends and enlarges thoracic cavity. Intra-thoracic pressure decreases. Air flows through tracheobronchial tree into the alveoli expanding lungs.
At a first glance, the mammalian resting breathing pattern appears to be an oscillatory event approximating a sinusoidal function, of which the amplitude is tidal volume (VT) and the period is the total breath duration (Ttot). In reality, a close look reveals major deviations from the sinusoidal function. For example, Ttot is not equally divided between the inspiratory and expiratory phases of the cycle, the inspiratory time (TI) being most commonly shorter than the expiratory time (TE). Also, the inspiratory phase of the Spiro gram is usually concave toward the time axis, whereas the expiratory phase is convex, occasionally with sudden interruptions of the expiratory flow [Fig.1]. Fig.1. Change in volume as function of time during breathing: Spirogram. On top, the corresponding changes in airflow (pneumotachogram). TI, inspiratory time. TE, expiratory time. TTOT, total cycle duration. VT, tidal volume. V, airflow.
The main components of the neuro-mechanical unit translating the neural output into a mechanical event. At left, some examples of mechanical constraints. Information about the changes in lung volume is fed back to the respiratory pattern generator mostly via activation of muscle proprioceptors and airways receptors ( chest wall and lung reflexes).
respiration is highly integrated with circulation allowing flexibility between individuals and between species in the best way to optimize gas exchange; control of depth and rate of breathing are essential components of respiratory control. Dyspnea :- non-specific symptom of many illnesses. the sensation is due to projections from the respiratory controller to higher centers, and projection of sensory information to the brainstem and cortex, and prior experience. the relation of dyspnea to the actual physiologic deficits is highly varied across cultures and individuals Þ relief of dyspnea may or may not correspond to adequate relief of the underlying physiologic causes. dyspnea can be due to physiologic mechanisms, cortical mechanisms, or a combination of both Þ the whole control system must be examined in the presence of dyspnea (from brain to lungs)
Metabolic Control: concerns O2 and CO2 (acid/base) balance; can briefly be overridden during speech, swallowing, etc., but metabolic control is always re-asserted after a minute or so; control at brainstem level. Behavioral Control: coordinates breathing with other complex voluntary functions (eating, talking, etc); control at thalamus and cortex; regulates use of motor systems used by both respiratory control and other activities. Reticular Activating System: links the BS and cortex to coordinate respiration with level of alertness (i.e. sleep/wake) Medullary Control: basic regulation occurs even when the cortex and mid-brain are separated from the medulla. breathing pattern is controlled by the nucleus tractus solitarius and the nucleus retroambiguus. rhythm generation occurs in the pre-Botzinger complex. proposed mechanism: tonic inspiratory drive comes from the dorsal motor group via phasic excitatory inputs; expiration is a result of reciprocal inhibition of the tonic drive (influenced by pneumotaxic center in the pons) apneusis: gasping, prolonged inspiration; occurs when pneumotaxic center is destroyed. neonates probably have an intrinsic respiratory pacemaker because tonic excitation/reciprocal inhibition systems may not yet be active.
higher brain centers (cortex, spinal, cerebellar): cortical outputs descend to the spinal neurons, and to the brainstem; lesions in certain areas of the brainstem can knock out metabolic control, but maintain volitional control (as long as the person is awake); cerebellum helps with coordination. spinal cord integration: descending impulses are modified by inter/intra-segmental neurons, and by motor reflexes integration is lost in a hiccup when the diaphragm is able to suck in the rib cage without reflexive activation of the intercostal muscles. receptors in the lungs: stretch receptors (smooth muscle layer), irritant receptors (epithelial cells), and un-myelinated C fibers (lung interstitium and alveolar walls) receptors in chest wall: joint, tendon, and muscle spindle receptors; reflex control is the same as other skeletal muscle, gamma motor neurons control the gain of the muscle stretch receptors.
causes of irregular breathing: CHF; CNS disease; sleep apnea; metabolic alkalosis; prematurity. causes of persistant hyperventilation: fibrotic lung disease; metabolic acidosis; CNS disorders (midbrain and pons); hepatic coma; ASA intoxication; fever; psychogenic. Cheyne-Stokes: alternating episodes of apnea and hyperpnea; instability of ventilatory control causes tidal volume to rhythmically increase and decrease; may occur in circulatory deficits because it takes extra time for the blood to equilibrate and the chemoreceptors may act inappropriately. may occur during hypoxia, sleep, high altitude, or after voluntary hyperventilation. Apneustic breathing: prolonged inspiration due to interruption of the pneumotaxic center (see above) Biot’s breathing: normal breathing interrupted by sudden apnea; may be a variant of Cheyne-Stokes. Ý breathing with hypocapnea: occurs when irritant or C-fiber receptors are activated (asthma, pulmonary embolus) Kussmaul’s breathing: hyperventilation with hypocapnea caused by acidosis (diabetic) hyperpnea of exercise: steady state of ventilation is achieved in 4-6 minutes with moderate exercise. ventilation first increases abruptly, then gradually, then reaches a steady state. mechanisms: cardiovascular mechanoreceptors; temperature receptors; chemoreceptors; mechanoreceptors in muscle; receptors monitoring metabolic activity.
lung disease often blunts the response to CO2 and O2; this can be due to increased effort required to breathe; decreased gas exchange; impaired muscle function; reduced responses to stimuli. causes of persistent hypercapnea: sleep apnea; CNS problems; metabolic alkalosis; myxedema; primary alveolar hypoventilation (Ondine’s curse - )spinal cord lesions; chest wall diseases; NM disorders; COPD.
Hypoventilation – an irregular and shallow pattern that may occur at any respiratory rate. Biots respirations :- an irregular, but cyclic pattern of an increased and decreased rate and depth, with long periods of apnea; it is associated with brain injury or heat stroke sometimes also called cluster respiration, is an abnormal pattern of breathing characterized by groups of quick, shallow inspirations followed by regular or irregular periods of apnea. It is distinguished from ataxic respiration by having more regularity and similar-sized inspirations, whereas ataxic respirations are characterized by completely irregular breaths and pauses.
Primary respiratory disorders : respiratory distress syndrome,brochopulmonary dysplasia. Infection/inflammation : pertussis, pneumonia, septicemia, meningitis bronchioloitis. Drug related: drug withdrawal. CNS: convulsion,intracranial intraventricular or subdural haemorrhage ,cerebral edema. GIT disorders: GERD. Cardic disorders:conginital heart diseases, conduction disorders(rare) Sleep apnea :enlarged tonsils, adenoids, extreme obesity(rare) , primary alveolar hypoventilation. Others: hypoglycemia, hypocalcemia.
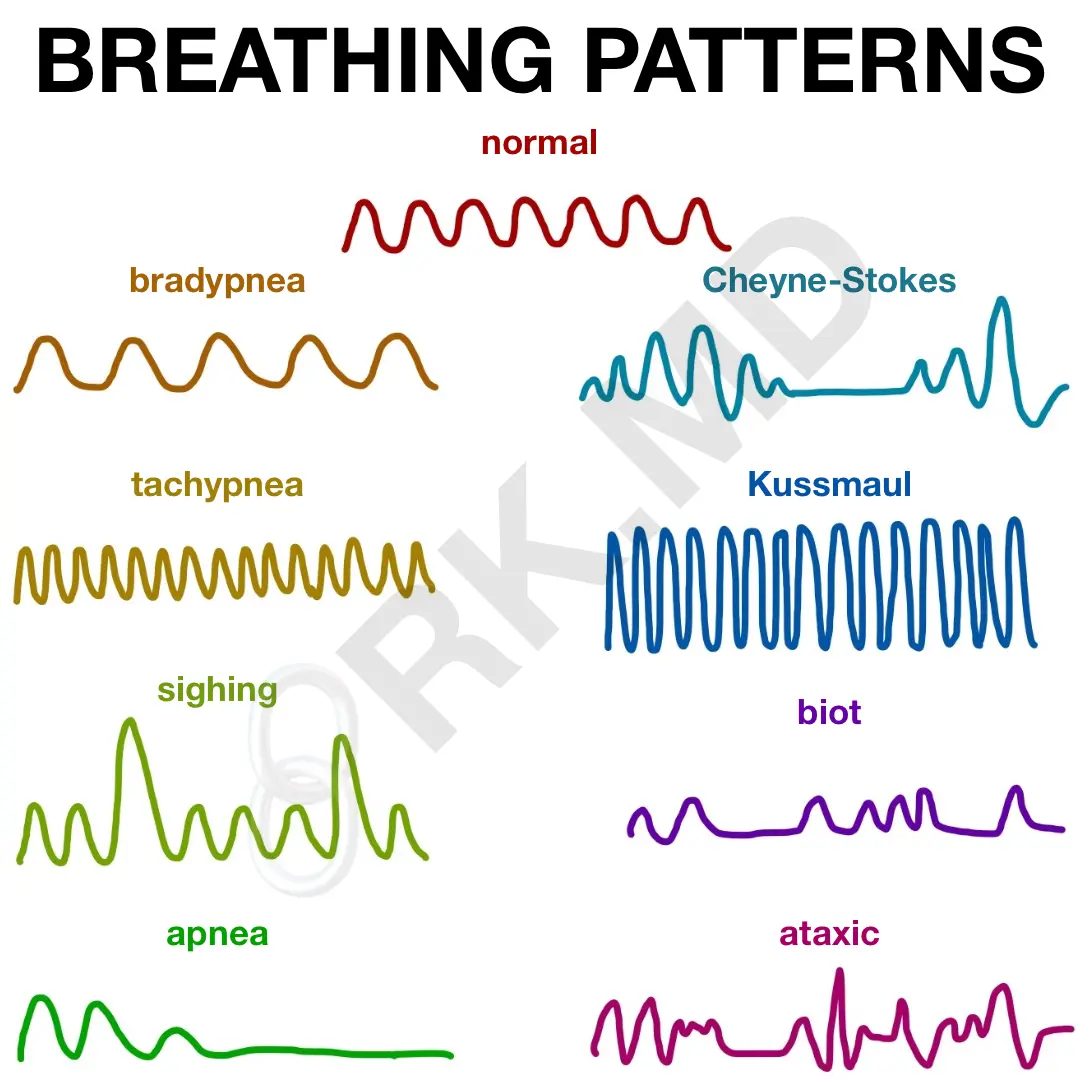
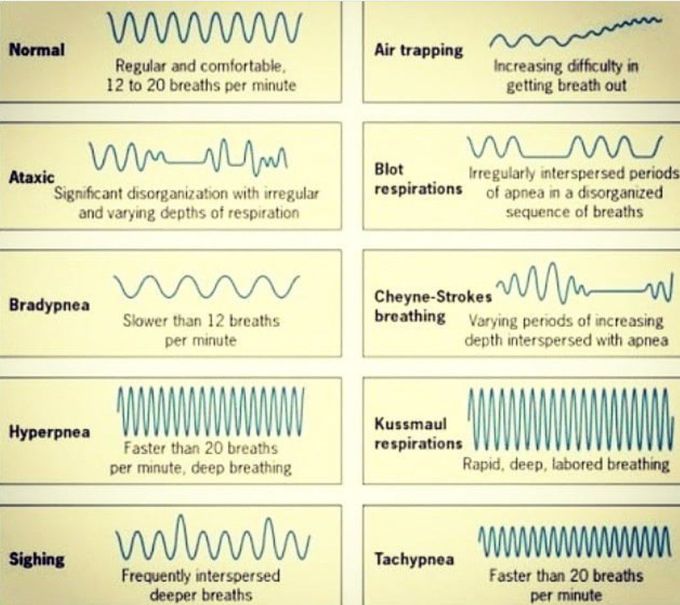
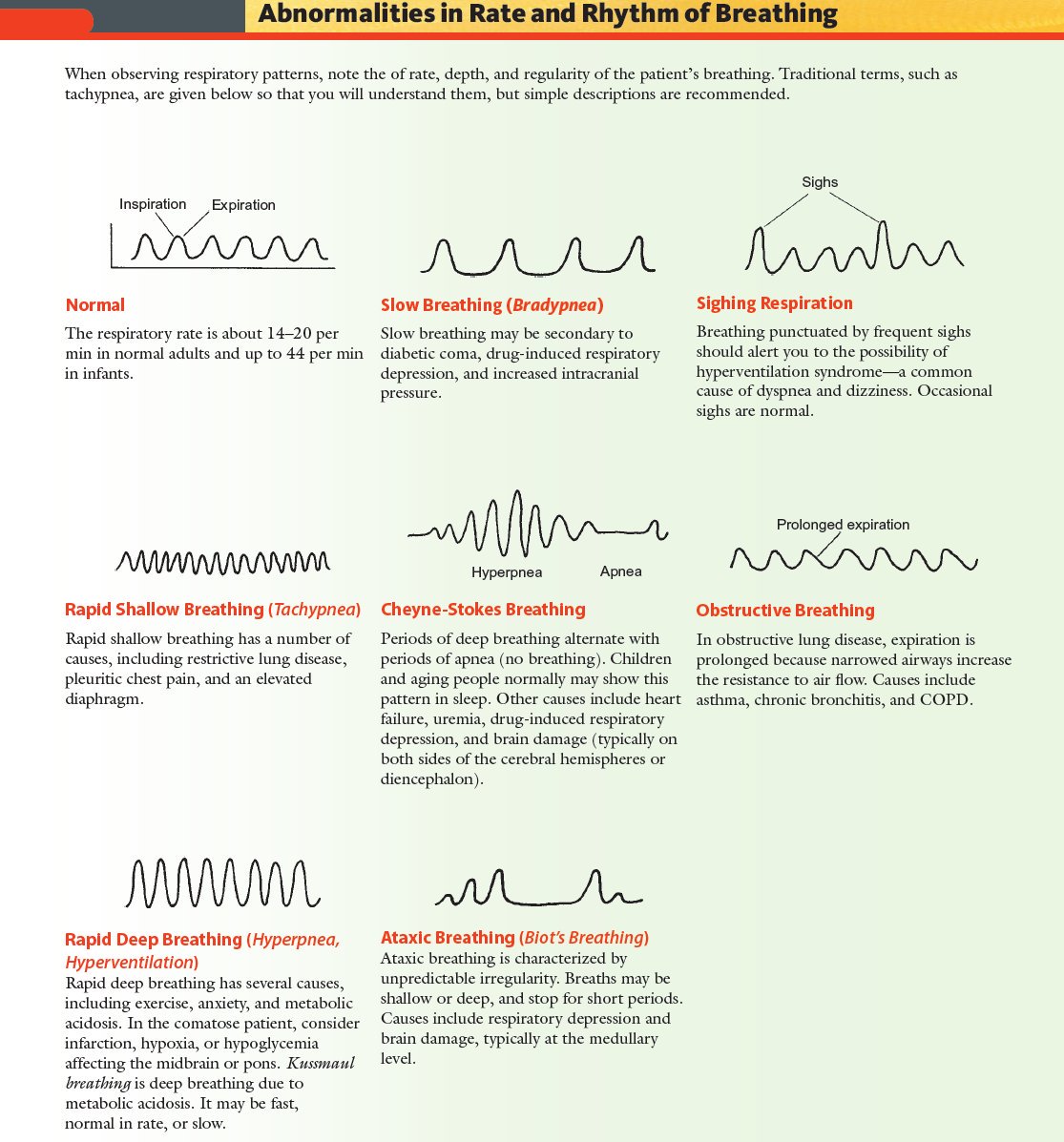
Eupnea – normal breathing. Tachypnea – rapid shallow breathing and the rate is age related. Hyperventilation – a rate greater than that required for normal body function; it is the result of increased respiratory rate, depth or both. Bradypnea – slow breathing.
Cheyne-Stokes respirations – a rhythmic pattern of gradually increase&decrease tidal volume interpersed with approximately equal periods of apnea (10-20 sec.) associated with severe CHF, increased ICP, drug OD or induced respiratory depression ,brain damage (strokes, head injuries or brain tumors and meningitis), uremia ,may be normal pattern of children during sleep, or adult sleep in high altitude . In cases of increasing intracranial pressure, it is often the first abnormal breathing pattern to appear. The condition was named after John Cheyne and William Stokes, the physicians who first classified it. This is caused by the failure of the respiratory center in the brain to compensate quickly for changing serum partial pressure of oxygen and carbon dioxide.. Cheyne-Stokes respirations are not the same as Biot s Respirations ( clusterbreathing ), where groups of breaths tend to be similar in size. .
Kussmaul breathing is named for Adolph Kussmaul, the 19th century German doctor who first noted it. It is also called air hunger . The cause of Kussmaul breathing is respiratory compensation for a metabolic acidosis, most commonly occurring in diabetics in diabetic ketoacidosis. Blood gases on a patient with Kussmaul breathing will show a low pCO2 because of a forced increased respiratory rate (blowing off the carbon dioxide). The patient feels an urge to breathe deeply, and it appears almost involuntary. The effect can be reproduced, to a degree, by rapidly breathing in the air in a recently-emptied plastic soft-drink bottle, which will normally contain a substantial amount of carbon dioxide..
This abnormal breathing is called agonal respiration and is the result of the brain s breathing center sending out signals even though circulation has ceased. The key point is that the abnormal breathing may sound like grunting, gasping or snoring. It disappears in 2-3 minutes. If you see this type of breathing DO NOT delay CPR. The person desperately needs air and only you can provide it. Agonal respiration is an abnormal pattern of breathing characterized by shallow, slow (3-4 per minute), irregular inspirations followed by irregular pauses. They may also be characterized as gasping, labored breathing, accompanied by strange vocalizations and myoclonus. Agonal breathing is an extremely serious medical sign requiring immediate medical attention, as the condition generally progresses to complete apnea and heralds death. The term is sometimes (inaccurately) used to refer to labored, gasping breathing patterns accompanying organ failure (e.g. liver failure and renal failure), SIRS, septic shock, and metabolic acidosis, or in general any labored breathing, including Biot s respirations and ataxic respirations. Correct usage would restrict the term to the last breaths before death..
Agonal respirations –ataxic breathing dying breaths :- characterized by continous irregular shifts of hyper/hypoventilation &apnea in no particular succession (unlike biotis &cheyne stoke) As the breathing pattern deteriorates, it merges with ataxic respirations. It is caused by damage to the medulla oblongata due to strokes or trauma or by pressure on the medulla due to uncal or tentorial herniation. It generally indicates a poor prognosis. Our greatest concern during this phase of the evaluation lies in the EMD’s ability to accurately assess the status of a patient’s breathing.
characterized by breathing abnormalities, intermittent disruptions of gas exchange, sleep interruption. Þ excessive daytime sleepiness, cardiac arrhythmias, behavioral abnormalities, Ý auto accidents; snoring (partial obstruction of the upper airway) is associated with HTN and stroke, possibly MI. Central Apnea: cessation of all breathing efforts. Obstructive Sleep Apnea most common disorder of breathing during sleep (2-4% of the population) breathing efforts persist but the upper airway is obstructed; partial arousal is important in terminating the apnea.
DI (desaturation index): number of times oxygen sat. falls by more than 4% AI (arousal index): number of arousals per hour (may or may not correlate with AHI) Treatment: should be geared towards the degree of disability, not the number of breathing disturbances. general: weight loss; relief of mechanical problems; don’t operate heavy machinery. CPAP (continuous positive applied pressure): prevents airway collapse and is effective in long-term treatment. dental prosthesis and electrical stimulation of the upper airway are currently being evaluated. correction of pathologic airways is beneficial remove enlarged tonsils, macroglossia, nasal polyps. uvulopalatopharynxgoplasty: 60% effective, but side effects suck (food regurgitation, speech problems) tracheostomy: bypass the problem; most successful, but again, the side effects suck. medical: little shown to be effective (weight loss is the most effective medical treatment)
When a patient is severely distressed modify questions to yes or no answers. Utilize family/caretakers, etc. Obtain OPQRST and SAMPLE information. .
NEED ORDERLY PROCESS. Before beginning, if possible: Quiet environment. Proper positioning (patient sitting for posterior thorax exam, supine for anterior thorax exam) Bare skin for auscultation. Patient comfort, warm hands and diaphragm of stethoscope, be considerate of women (drape sheet to cover chest) Inspect. Palpate. Percuss. Auscultate.
Observe the patient’s breathing pattern. Rate (normal vs. increased/decreased) Depth (shallow vs. deep) Effort (any sign of accessory muscle use, inspect neck) Assess the patient’s color. cyanosis.
Infant Toddler Preschooler School-age child Adolescent Adult
Administer oxygen via a nonrebreather mask at a flow rate sufficient to keep the reservoir bag inflated: during inspiration, usually requires a flow rate of at least 12 liters/minute and may require 15 liters/minute.
When spontaneous breathing is present but ineffective, the following may indicate a life-threatening condition related to breathing: Altered mental status (i.e. restless, agitated) Cyanosis, especially around the mouth. Asymmetrical expansion of the chest wall. Use of accessory and/or abdominal muscles. Sucking chest wounds. Paradoxical movement of chest wall during inspiration and expiration. Tracheal shift from the midline position.
Ventilate the. Patient via a bag-valve-mask device with an attached oxygen reservoir system 100% Assist with endotracheal intubation: ventilate with oxygen via a bag-valve device attached to an oxygen reservoir system.
Life-threatening compromises in breathing may occur with a history of any of the following: Blunt or penetrating injuries of the thorax. Patient striking the steering column or wheel. Acceleration, deceleration, or a combination of both types of forces (e.g., motor vehicle crashes, falls. crush injuries)
Chest rise and fall (depth and symmetry) Skin color. General respiratory rate • Normal • Slow • Fast. Pattern of breathing • Regular • Irregular • Cheyne Stokes. Integrity of the soft tissue and bony structures of the chest wall. Use of accessory and/or abdominal muscles. Bilateral breath sounds: Auscultate the lungs bilaterally at the second intercostal space midclavicular line and at the fifth intercostals space at the anterior axillary line. Jugular veins and position of trachea.
R – region/referral/radiation. S – severity. T – time.
P – pertinent past medical history. L – last oral intake. E – events leading up to.
A patient with moderate to severe distress will have difficulty speaking in full sentences. The inability to speak in full sentences indicates an immediate life threat. A limited number of words spoken between breaths is described as one, two, or three word dyspnea.
Other findings that indicate an immediate life-threat in a patient with respiratory distress include: Altered MS, anxiety or confusion/hypoxia. Signs of poor perfusion such as cyanosis, pallor, or diaphoresis. Absent or abnormal breath sounds. Use of accessory muscles. Tachycardia or bradycardia (sustained) Hypotension.
Nasal flaring – widening of the nostrils indicates partial airway obstruction, most notable in children. Carpopedal spasms – spasmotic contractions of the hands, wrists, feet, and ankles from prolonged hyperventilation or any condition that leads to respiratory alkalosis.
One or two word dyspnea = severe distress. Purses-lip breathing – creates airway pressure to help keep the alveoli from collapsing. Retractions – accessory muscle use, most notable during inspection (ribs, clavicles, sternum)
When assessing breath sounds: Listen to skin not the shirt! Apex to base comparing side-to-side. Use simple terms to describe your findings.
Wheezing – continuous whistling sound caused by narrowing of the lower airways. Stridor – is a disturbing high-pitched sound associated with upper airway obstruction. Grunting – is a sound that occurs primarily in infants/small children when the child breathes out against a partially closed epiglottis (usually a sign of distress)
Absent unilateral sounds may be due to pneumothorax, pneumoectomy, increased consolidation (pneumonia) decompensated COPD or partial FBAO. Pleural friction rub – is not a lung sound but is heard in the chest as a grating sound over the area that is painful.
Apneusis: respiration ceases in inspiratory position, because of sustained contraction of the inspiratory muscles. Biot s Respiration: sequences of uniformly deep gasps, apnea, then deep gasps. Breath-holding: voluntary apnea, either by continuous contraction of the inspiratory muscles, or by relaxation against glottis closure. Cheyne-Stokes Respiration: cycles of gradually increasing tidal volume followed by gradually decreasing tidal volume, usually separated by brief periods of apnea. Dyspnea: difficult or laboured breathing; an uncomfortable awareness of the act of breathing, air hunger . Eupnea: normal spontaneous breathing. Hyperpnea: increased pulmonary ventilation (above the normal resting value)
Hypopnea: ventilation below the normal level. Hypoventilation: ventilation less than required by metabolic demands, irrespective of the absolute value of ventilation. Orthopnea: dyspnea experienced only in the recumbent position, usually supine, and relieved by sitting or standing. It often occurs in patients with left ventricular insufficiency. Panting: breathing pattern both very rapid and shallow. In some conditions, this pattern is adopted to dissipate heat (thermal panting). Periodic breathing, abnormal breathing pattern, with a series of cycles separated by pauses. Tachypnea: increased rate of breathing.
Dyspnea from pulmonary causes tend to resolve quicker with cessation of exertion than cardiac causes. Causes of dyspnea without exertion include: anemia, chest trauma, acute MI, pulmonary embolism, spontaneous pneumothorax.
Acute dyspnea in the elderly is often caused by exacerbation of COPD or heart failure.
Infection. Allergies. Tobacco smoke. Chemicals or other irritants. Medications may worsen COPD (ie: beta-blockers)
The management of a patient with a respiratory problem includes a prompt and accurate assessment with recognition of immediate life-threatening conditions, followed by prompt intervention and resuscitation as appropriate. When the patient’s condition is unstable or critical these steps take priority over a detailed assessment.
Ask the most pertinent questions first. Be alert for signs of rapid deterioration and quickly formulate a plan to intervene. Many patients with dyspnea are having a cardiac problem. The assessment process is dynamic and the EMS provider must modify the FH & PE to include more than one body system.

Lung histopathology slides. Lung histopathology is shown in the
8 Guillain-Barre Syndrome Nursing Care Plans - Nurseslabs
Breathing patterns
Pathological breathing / Abnormal breathing patterns : Kussmaul

Breathing patterns
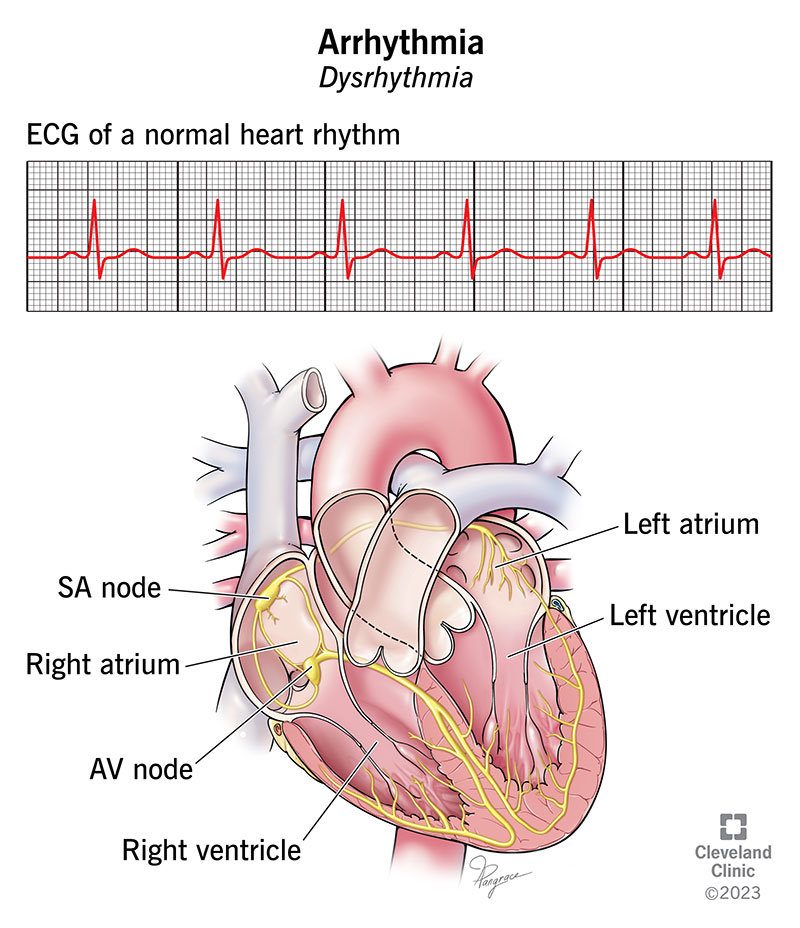
Arrhythmia: Symptoms & Treatment
PPT - Breathing Patterns PowerPoint Presentation, free download
Basics of volumetric capnography - Part 3: Clinical relevance
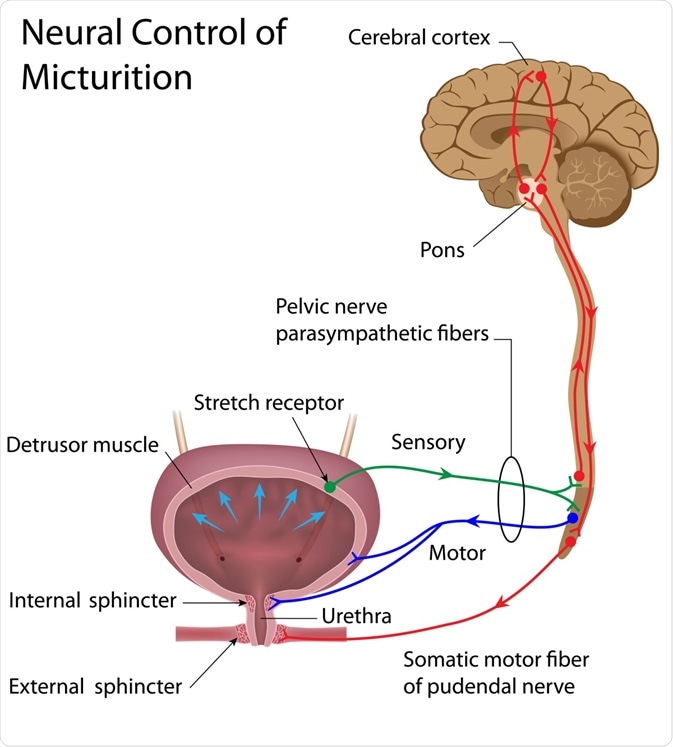
Micturition Reflex - Neural Control of Urination
PPT - Breathing Patterns PowerPoint Presentation, free download

Vital Signs: Basic Physical Exam Terminology - Lesson

RNA interference - Wikipedia